


TLV to implement varying cost-effectiveness thresholds depending on patient volumes
TLV communicates that patient volumes will explicitly be considered when assessing a reasonable cost per QALY

Yes, a first post in English. Going forward, Pharmaekonomi will be a bilingual substack, mixing posts in Swedish and English. This first English post is written in collaboration with NHTA Sweden.
In Swedish prescription drug reimbursement decisions by TLV, it is well established that the highest acceptable cost per QALY (ICER) is dependent on the severity of the disease. Although TLV has never published any formal ICER thresholds, it is often considered that a drug targeting a non-severe disease must be priced so that the ICER comes in below (about) 0.5 million/QALY. In contrast, a drug targeting a (very) severe disease is often reimbursed at ICERs up to 1 million/QALY. The thresholds are very influential in the final reimbursement decision. For example, many cancer drugs with an ICER below 1 million/QALY are reimbursed, whereas the likelihood of reimbursement drops substantially as soon as the ICER exceeds 1 million/QALY.
There has been a long-standing discussion about other criteria besides severity that should affect the cost-effectiveness threshold, often centered around how to assess orphan drugs. TLV has now explained that they aim to consider patient volumes when evaluating a reasonable cost per QALY. Chief economist at TLV, Douglas Lundin, has expressed that a higher ICER threshold will be accepted for drugs targeting very rare diseases, whereas a lower ICER threshold will be required for drugs targeting common diseases.
A cost-effectiveness approach that uses the same threshold for all conditions can be motivated by the aim of maximizing population health with a given budget. In such a framework, having the same “willingness” to pay per QALY for all new drugs makes sense. By allowing a higher ICER threshold for orphan drugs, we “lose more population health than we gain”. However, this “pure” efficiency criterion does not seem to have widespread support, and other criteria based on non-utilitarian principles have been used to argue for different decision criteria for across diseases, including arguments that no patient group should be “abandoned” simply due to a disease being very rare.
The underlying economic challenge with orphan drugs is that the semi-fixed Research & Development (RD) costs can only be distributed across a small patient group, which makes it more difficult to financially motivate R&D investments in rare diseases. Many countries have tried to address this by implementing a number of incentive systems for rare diseases, including tax breaks and “easier” regulatory approval processes. This has generally been very successful, and there has been a rapid increase in the number of orphan drugs coming to the market and orphan drugs now account for a substantial share of global pharmaceutical sales. Despite orphan drugs being markedly more expensive, estimates suggest a price difference of 5x, it is actually not clear that orphan drugs have a more challenging time reaching a positive outcome in conventional cost-effectiveness analyses. One study from NICE decisions in the UK found a somewhat similar positive recommendation rate for orphan and non-orphan drugs.
However, TLV has now suggested an amendment to the cost-effectiveness framework that will explicitly consider rarity/volume. The suggestion is a “staircase”-model where the highest acceptable cost per QALY may reach a few million per QALY in a setting with a very rare disease, with very high severity, and clinically meaningful patient benefits.
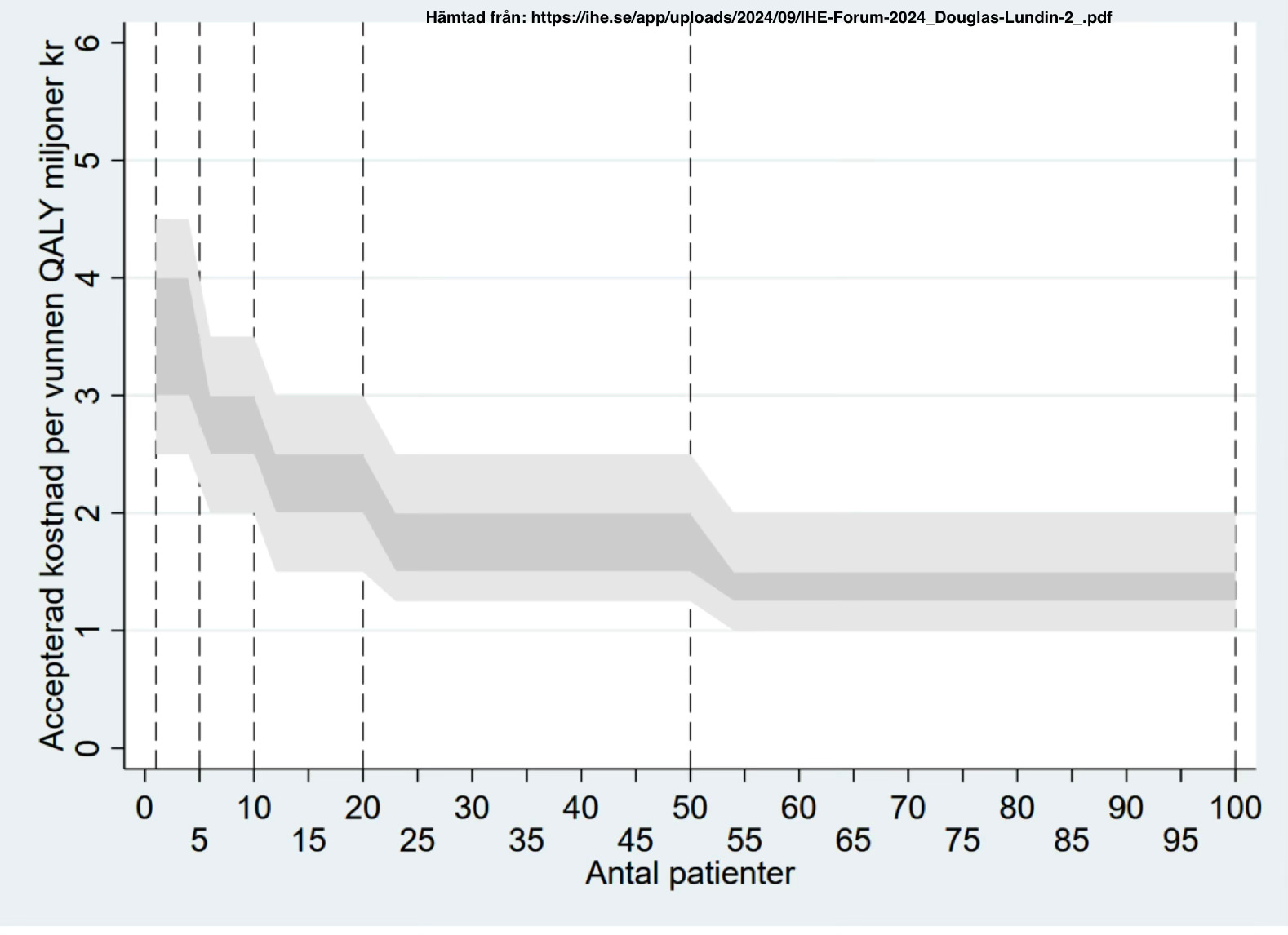
In parallel, for drugs with an indication that allows for a very large patient population, the message from TLV is that a lower ICER threshold will be applied. This could be achieved by requiring a lower ICER threshold at the time of the reimbursement decision or by having mandated discounts if the producer reaches certain sales volumes.
It remains to be seen how patient volumes will affect price-setting criteria at TLV in practice. Still, it seems clear from TLV messaging that there will be a more explicit variation in the accepted cost per QALY depending on patient volumes.